Eye Surgery
 |
| Intraocular lens Illustrations | |
 |
 |
| Phakic IOL anterior chamber, intraocular lens implant. | Phakic IOL posterior chamber, sulcus, implant. |
 |
 |
| Phakic IOL implant. | Piggyback IOL implants |
 |
 |
| Soft, foldable Intraocular plate lens implant illustration. | Phakic IOL for posterior chamber, sulcus. |
 |
 |
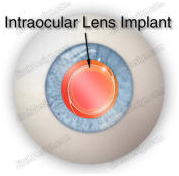
| Soft, foldable intraocular plate lens, IOL. | IOL, intraocular lens implant illustration. |
 |
 |
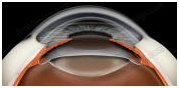
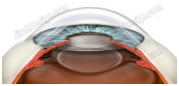
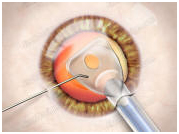
| Intraocular lens implantation surgical illustration. | Intraocular lens implant, IOL, cross-section view. |
 |
 |
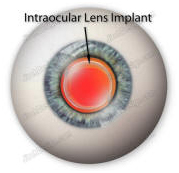
| Intraocular lens implant illustration with eyeball. | Intraocular lens implant illustration, IOL, 3-piece |